Yeap but it is HEAVILY moderated...you have to toe the party line. And I don't do that too well. But I stay cause others may need a voice of reason!I've always just called it the DS. But I know on my surgery report he put BPD with DS. I didn't know he had his own group.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Dr. Stephen Boyce/Knoxville, TN
- Thread starter southernlady
- Start date



Help Support Bariatric & Weight Loss Surgery Forum:
jjordan8130
Well-Known Member
Thank you guys! I appreciate the info! Dr. Housten does the DS.....no BPD. He did say he would rather sleeve someone and DS them later for non complience than to just DS them in the beginning. He anticipates a lot of DS revisions after sleeve fail from all the patients he's operating on now. I feel confident he will do a good job. He asked me how long I wanted my common channel and suggested 100cm. But I was leaning toward a little longer like the 120-150 range.
Have any of you tried the Barilife vits?? I'm interested in the powder version? A friend of mine and fellow DS'r swears by it. Trying to plan ahead and decide on what vit regimen I'd like to try post op. Thoughts? Advice? I've looked at vita lady, but I'm a person that struggles with pills. It's such a battle for me to take my daily reginmen now because I get sick.
Have any of you tried the Barilife vits?? I'm interested in the powder version? A friend of mine and fellow DS'r swears by it. Trying to plan ahead and decide on what vit regimen I'd like to try post op. Thoughts? Advice? I've looked at vita lady, but I'm a person that struggles with pills. It's such a battle for me to take my daily reginmen now because I get sick.
Stay AWAY from the BariLife...waste of money. Stick with vitalady. If you struggle with pills you can cut/crush or just open the pill casing on things like the D. It's easier to come down from levels too high than to get them out of the toilet.Thank you guys! I appreciate the info! Dr. Housten does the DS.....no BPD. He did say he would rather sleeve someone and DS them later for non complience than to just DS them in the beginning. He anticipates a lot of DS revisions after sleeve fail from all the patients he's operating on now. I feel confident he will do a good job. He asked me how long I wanted my common channel and suggested 100cm. But I was leaning toward a little longer like the 120-150 range.
Have any of you tried the Barilife vits?? I'm interested in the powder version? A friend of mine and fellow DS'r swears by it. Trying to plan ahead and decide on what vit regimen I'd like to try post op. Thoughts? Advice? I've looked at vita lady, but I'm a person that struggles with pills. It's such a battle for me to take my daily reginmen now because I get sick.
BrianChesteen
Glad to be a Loser!
The Barilife powdered vits are like trying to eat sand. The taste is horrible. Think instant gag reflex. How people take this stuff post op is beyond my comprehension!
I will let the vets respond (and I know they will) about how well the all in one multi vit regimens work for a DS'er long term.
I will let the vets respond (and I know they will) about how well the all in one multi vit regimens work for a DS'er long term.
jjordan8130
Well-Known Member
WOW!!! OK!! Looks like I need to revisit vitalady! Barilife just seemed SO appealing. ") Thank you!!!
Thank you!!!
Thank you!!!An all in one SOUNDS appealing but it works out SO badly for most of us.WOW!!! OK!! Looks like I need to revisit vitalady! Barilife just seemed SO appealing.
Example, I have to take 50,000 IU of Dry D3 every day and 100,000 IU two days of the week. I need 2,000 units of K1 daily.
I do NOT need extra A or E but if I used the BariLife, I would need 17 pills a day on my "light" days to get enough vit D and 34 pills twice a week.
IF I did that, I would end up getting 85,000 IU of A which is WAY above what I need. I do fine with MY A taking just three Kirkland Daily multi's...and I get 500 of those for less than $15.00 which comes out to less than a dime a day in multis. And will last me well over three months. The BariLife costs over .15 cents a pill and I would need 17 a day to the tune of $2.55 a day and still have to suppliment versus the dime I spend now and add the vitamins *I* need.

$10.17
$18.99
The Complete Bariatric Cookbook and Meal Plan: Recipes and Guidance for Life Before and After Surgery
Amazon.com










$18.70 ($1.65 / Ounce)
$19.99 ($1.76 / Ounce)
Quest Nutrition Mini Cookies & Cream Protein Bars, 8g Protein, 1g Sugar, 2g Net Carbs, Gluten Free, 14 Count
Amazon.com

$16.99 ($0.39 / Ounce)
BariWise Protein Soup Mix, Chicken Noodle, 15g Protein, Low Carb (7ct).
DIET DIRECT




$10.00 ($10.00 / Count)
First Days Maternity - Maxi Peri Bottle for Maximum Postpartum Soothing! Large 650ml Capacity Allows for an Effective Soothe. Pink Colour
First Days Maternity






$9.49
$15.99
Fresh Start Bariatric Cookbook: Healthy Recipes to Enjoy Favorite Foods After Weight-Loss Surgery
Amazon.com

$41.00
Walttools Tru Tex CORAL Texture Roller Sleeve for Concrete Flatwork and Vertical Concrete - Quick, Easy, Realistic Patterns, User-Friendly (Coral Stone)
Decorative Concrete Supply Source





$44.75 ($1.23 / Ounce)
$54.75 ($1.50 / Ounce)
LIVING HEALTHY NUTRITION BariSuccess Vanilla Whey Isolate Protein Powder - 30g Protein, 30 Servings/Container - Free of Fat, Sugar, Gluten, Soy & Lactose - Low Carb Bariatric Meal Replacement Protein
My Bariatric Kitchen

$8.99
$15.99
The Gastric Sleeve Bariatric Cookbook: Easy Meal Plans and Recipes to Eat Well & Keep the Weight Off
Amazon.com




$11.36
$14.95
Gastric Bypass Diet: Step By Step Guide to Gastric Bypass Surgery (Bariatric Cookbook)
Amazon.com




$19.87 ($0.17 / Count)
$29.97 ($0.25 / Count)
PAWFECTCHEW Pawfect Mobility - Glucosamine Treats for Dogs - Hip & Joint Health Supplement Chews w/Omega-3, Chondroitin, MSM - Made in USA - Joint Pain Relief - Hip & Joint Care - 120ct
PawfectSupplies


$9.29
$14.95
Gastric Bypass Recipes: 80+ Simple Recipes for the First Stage After Gastric Bypass Surgery (Bariatric Cookbook)
Amazon.com

Stephanie Hazel
New Member
- Joined
- Sep 27, 2014
- Messages
- 4
Yeap but it is HEAVILY moderated...you have to toe the party line. And I don't do that too well. But I stay cause others may need a voice of reason!
** Is his group within bariatric facts or another website? I would like to follow that as well, just for informational purposes. Thx!!
His group is on facebook. And while it is a closed group, you can find it: https://www.facebook.com/groups/126366992588/** Is his group within bariatric facts or another website? I would like to follow that as well, just for informational purposes. Thx!!
Edited: his group is now closed as he has retired.
Last edited:
Stephanie Hazel
New Member
- Joined
- Sep 27, 2014
- Messages
- 4
Thanks so much for that!! Will go find that group now.
Barb1
Well-Known Member
Just my 2 cents but I think for coding for insurance approval it says BPD/DS. I am sure this causes confusion for some when they see their EOB or bill from the hospital.
Even in your insurance information it usually says BPD/DS.
I like the fact the Dr. Boyce is training other surgeons to do the DS. To me that gives him extra points.
Even in your insurance information it usually says BPD/DS.
I like the fact the Dr. Boyce is training other surgeons to do the DS. To me that gives him extra points.
Susan in Tennessee
Well-Known Member
Yep. Dr. Boyce does the modern DS and does call it the BPD-DS most of the time.
I have been getting confused in my research on this point as well! After SouthernLady mentioned Dr. Boyce in Knoxville I was reading on his website and found it VERY confusing. Under the tab "WLS options" it shows (if I am remembering correctly) BPD, BPD with DS and DS??? along with all the others. From reading on here from people who have had him as a surgeon, when they say DS it's the full DS with the sleeve stomach (that leaves pyloric intact) and shortened other stuff (that was technical, huh?). Why in the world would they keep the wording so confusing on the sight?
Also in my reading here of the back threads I saw someone wondering aloud if BLIS insurance covered DS anywhere. According to my reading on Boyce's site it sounds as if BLIS coverage is included in the $25,750.00 quoted there as a pre-pay amount. What I wasn't sure about was whether a program fee that I saw mentioned was something above and beyond this $25,750.00 or if it was included. I haven't made any calls to anyone's office yet as I'm still doing my own research to know what I do want and need to ask when I do talk to someone.
Other things I will find out are whether he uses the Hess method in determining length to use and if he'll consider me for DS. From the voices of experience here, I'm very interested in hearing if Hess method is best. If a surgeon does NOT use that method to determine length what does he use...a set one size does all, or take into account background history, lifestyle, etc? I started to say "his gut feeling" but decided not to"!
The ease of having a surgeon stateside, even within approximately 130 miles of home sounds really great, but the monetary aspect is huge too. I know Ungston is no longer doing the DS but it sounds like Dr. Esquerra is doing well and the difference would be at least 10k. Does anyone have any info to the contrary of Dr. Esquerra doing commendable work?
I've been trying to go through the back posts and find answers to questions and I do apologize if I'm asking things that have been asked a million times. I'm not the greatest at navigating the board yet. I do appreciate the expertise here and everyone's willingness to help.
BebeZed
Well-Known Member
- Joined
- Sep 8, 2015
- Messages
- 507
The ease of having a surgeon stateside, even within approximately 130 miles of home sounds really great, but the monetary aspect is huge too. I know Ungston is no longer doing the DS but it sounds like Dr. Esquerra is doing well and the difference would be at least 10k. Does anyone have any info to the contrary of Dr. Esquerra doing commendable work?
I had originally wanted Dr Ungson to perform my DS, but unfortunately between the time I made my inquiries and the time I was ready to schedule, Dr Ungson had already been offered and accepted his government position. I went into total panic mode; a couple of us were scheduled and we had next to NO information. I contacted Nina at MBC and found out that Esquerra had worked with Ungson for several years, had trained him, and turned over his private practice to him when he accepted the government position. I then went on a research binge to verify the relationship between Ungson and Esquerra and was able to confirm - they worked together in both Hermosillo and Mexicali. I then tried to find any negative things about Dr Esquerra and didn't find anything... and since I was going to be the 2nd in line from this community to go under his knife, I definitely was looking for ANYTHING, good or bad. Couldn't find anything bad at all. And I was really truly looking because at that point nobody here was familiar with him.
Yeah, it IS confusing but many surgeons, not just Boyce call it the BPD/DS.Under the tab "WLS options" it shows (if I am remembering correctly) BPD, BPD with DS and DS??? along with all the others. From reading on here from people who have had him as a surgeon, when they say DS it's the full DS with the sleeve stomach (that leaves pyloric intact) and shortened other stuff (that was technical, huh?). Why in the world would they keep the wording so confusing on the sight?
Okay, the BPD is NOT a DS but has a pouch instead of a sleeve.
The BPD/DS is the "guts" of the BPD but the sleeve instead of a pouch.
The DS is what most DS'ers call it because we HATE that the BPD is attached and confusing medical personnel that hear "BPD" part of the BPD/DS and tune out the rest. The BPD is not commonly done and is NOT a standard of care operation.
http://www.dsfacts.com/history-of-duodenal-switch.php
Biliopancreatic Diversion (BPD)
Dr. Nicola Scopinaro introduced the Biliopancreatic Diversion in Italy during 1979.The procedure combines malabsorption with some gastric restriction. A large pouch between 250 and 400 ccs is created with the upper portion and the lower stomach is surgically removed (distal gastrectomy). The pyloric valve is circumvented so "dumping" often occurs. The duodenum (top part of the small intestine) is bypassed and the stomach pouch is connected to the lower 2-3 meters of the small intestine. Then, 4-metres of the small bowel (60%) is bypassed making the channel approximately 50 cm.
Stand-Alone Duodenal Switch
The Stand-Alone Duodenal Switch procedure (without the accompanying gastric bypass as used in weight-loss surgery) was developed by Dr. Tom R. DeMeester in the 1980's to treat bile-reflux gastritis, a condition in which the stomach and esophagus are irritated by bile that goes back through the pylorus to the stomach.
Biliopancreatic Diversion with Duodenal Switch (BPD-DS)
In 1986, Dr. Douglas Hess modified BPD and combined it with Duodenal Switch. This hybrid procedure is often referred to as the Biliopancreatic Diversion with Duodenal Switch, or GR-DS (Gastric Reduction- Duodenal Switch). Keep in mind; the BPD portion has been modified from the original procedure so the name can be misleading.
Duodenal Switch (DS)
DS surgeons and patients commonly refer to this procedure as the Duodenal Switch. Hess's Duodenal Switch has the advantages of the BPD, but without some of the associated problems like marginal ulcers, stoma closures and blockages, dumping syndrome, and serious protein-calorie malnutrition; all of which can occur after other gastric bypass procedures.
Picture of the BPD: Notice the LARGE pouch and the missing pyloric valve.
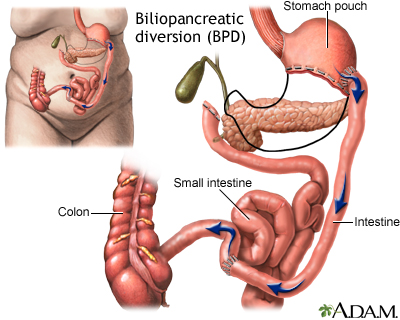
And this is the DS (BPD/DS). Notice it's a sleeve WITH the pyloric valve.

I get terribly frustrated with Boyce's office and FB page cause people are always "shortening" the BPD/DS to BPD and it is NOT the same. We try to explain when we can that using the proper term will help them in the future with medical personnel NOT versed in bariatric surgery.
But on his site, using the term BPD/DS is technically correct even if not LOGICALLY correct.
To MY knowledge, he does not use the Hess method. At the time I had my surgery, I didn't know enough to challenge that but I would now. He DID take my BMI into account when he did mine. I got a super tiny sleeve and a longer than typical common channel.Other things I will find out are whether he uses the Hess method in determining length to use and if he'll consider me for DS. From the voices of experience here, I'm very interested in hearing if Hess method is best. If a surgeon does NOT use that method to determine length what does he use...a set one size does all, or take into account background history, lifestyle, etc? I started to say "his gut feeling" but decided not to"!
Susan in Tennessee
Well-Known Member
Thanks! Good to hear that.I had originally wanted Dr Ungson to perform my DS, but unfortunately between the time I made my inquiries and the time I was ready to schedule, Dr Ungson had already been offered and accepted his government position. I went into total panic mode; a couple of us were scheduled and we had next to NO information. I contacted Nina at MBC and found out that Esquerra had worked with Ungson for several years, had trained him, and turned over his private practice to him when he accepted the government position. I then went on a research binge to verify the relationship between Ungson and Esquerra and was able to confirm - they worked together in both Hermosillo and Mexicali. I then tried to find any negative things about Dr Esquerra and didn't find anything... and since I was going to be the 2nd in line from this community to go under his knife, I definitely was looking for ANYTHING, good or bad. Couldn't find anything bad at all. And I was really truly looking because at that point nobody here was familiar with him.
Clematis
Well-Known Member
- Joined
- Sep 5, 2015
- Messages
- 1,705
Ditto what bebezed said. Esquerra and Mexicali Bariatric Center was great. The DS was $11k all included, including transportation to/from San Diego and hotel the night before surgery. I added on a $2k gallbladder removal.
When I looked into BLIS (for US surgeons) on the BLIS website, I did NOT see that it covered the DS.
I don;t think there is any international complication insurance for Esquerra/MBC, however they will take care of whatever goes wrong (you have to get there, though) and your only costs are the hospital fee which is next to nothing in MX.
When I looked into BLIS (for US surgeons) on the BLIS website, I did NOT see that it covered the DS.
I don;t think there is any international complication insurance for Esquerra/MBC, however they will take care of whatever goes wrong (you have to get there, though) and your only costs are the hospital fee which is next to nothing in MX.